Children with Chronic Conditions
Children with Chronic Conditions 2
 photo")
Nicola Brodie, MD (she/her/hers)
Pediatrician
Children's National Health System
Washington, District of Columbia, United States
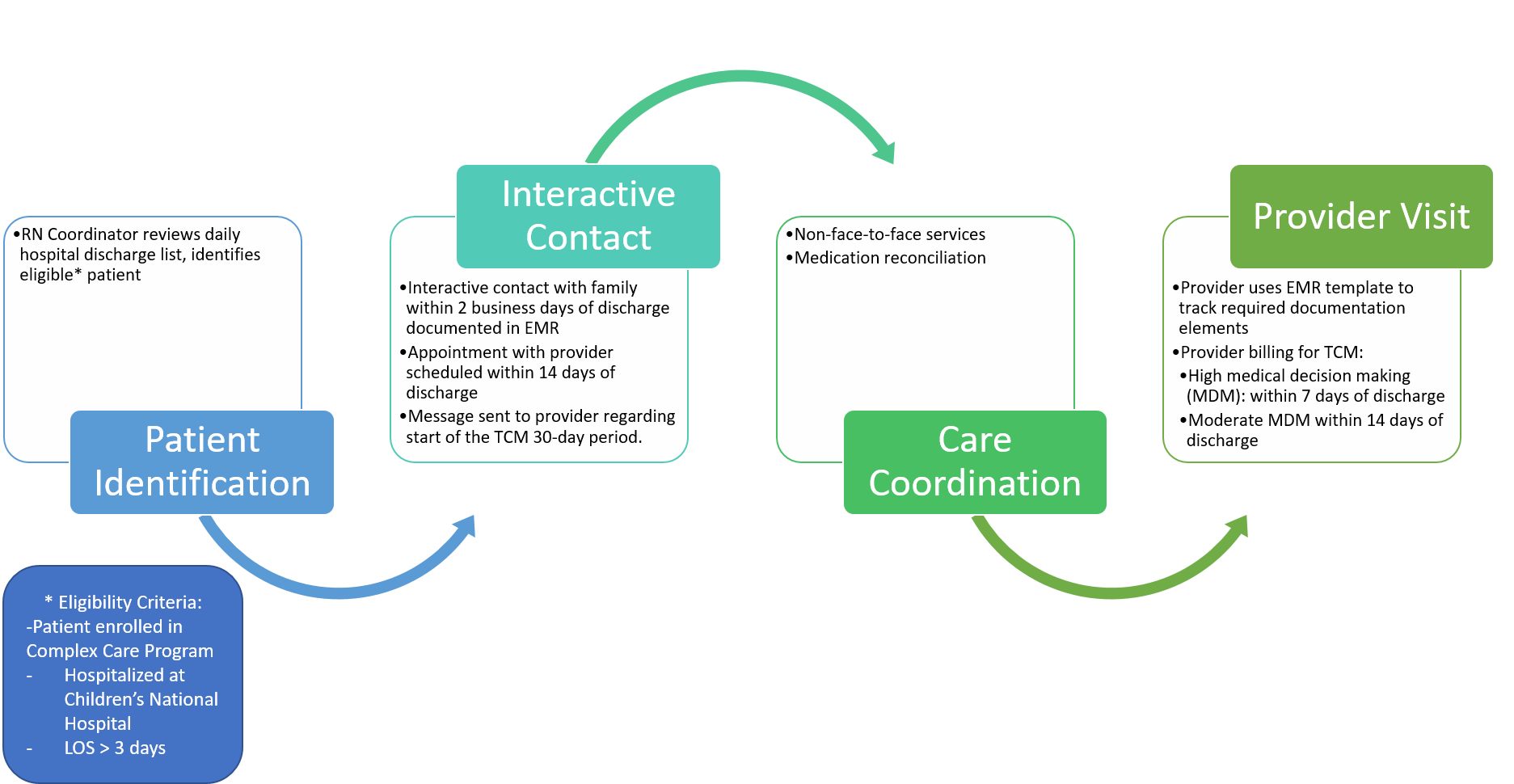
A nurse from our program provided outreach to patient families within two business days of discharge to assess for any urgent transitional needs (equipment, medication, or unanswered questions) and to schedule a post-hospitalization visit with the patient’s primary care provider within 14 days of discharge. After the visit with the provider, the TCM CPT code was used to capture the bundle of transitional care services provided (Figure 1). Reimbursement data from our payors was obtained.
Results:
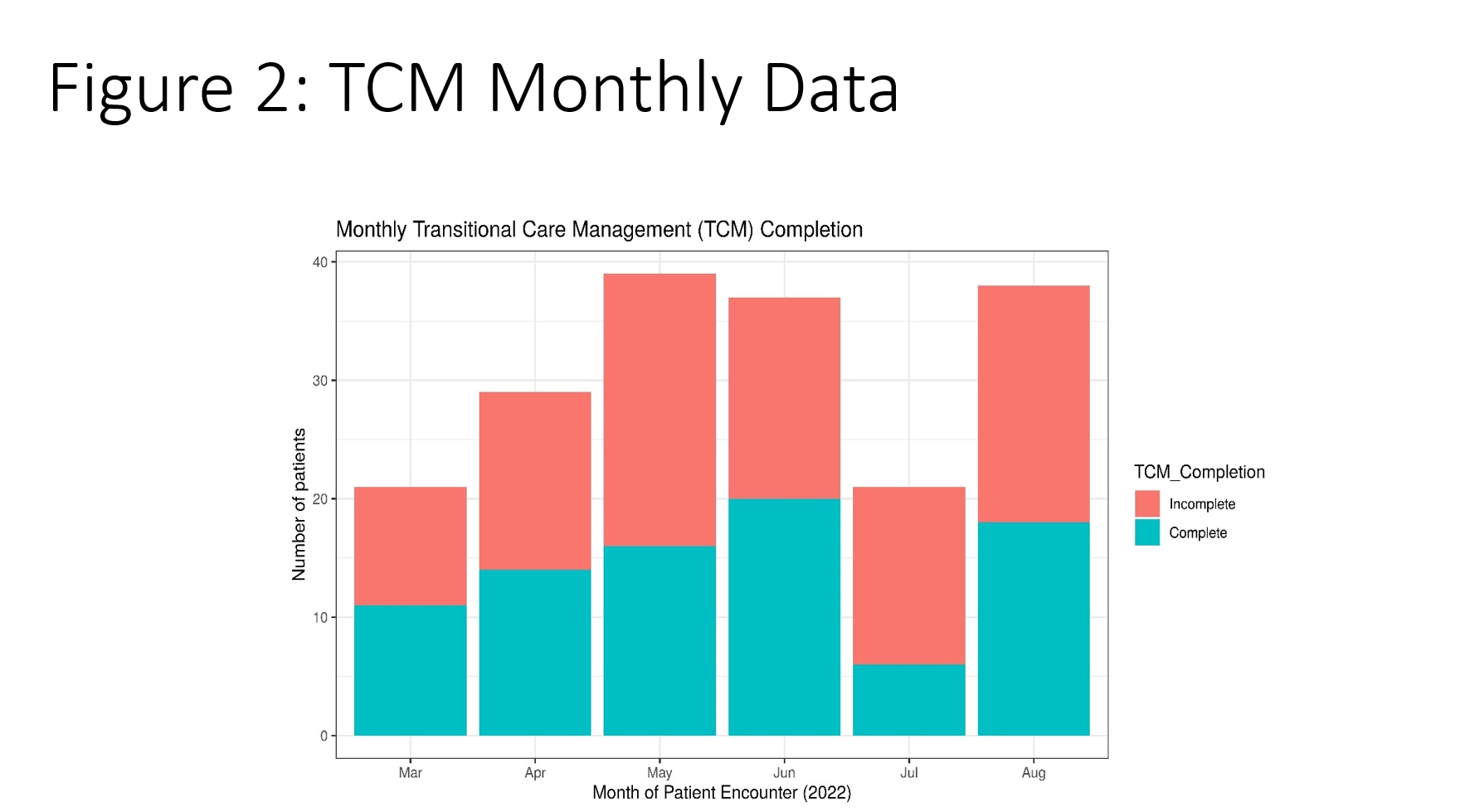
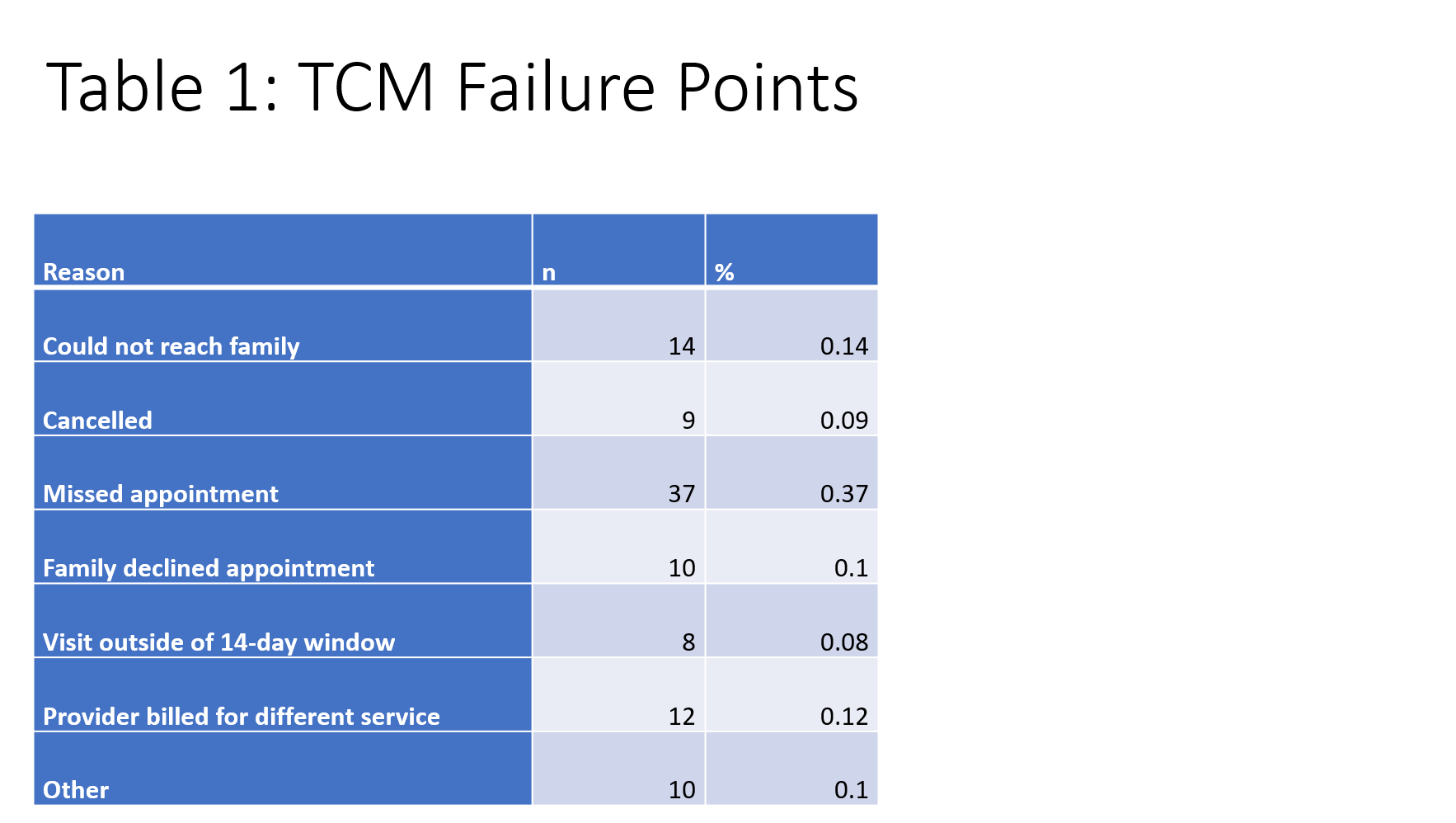
During our six-month pilot period, a total of 185 discrete encounters were identified as eligible for the TCM process; of these, 93 successfully completed the process with all required elements (50%); monthly data is shown in Figure 2. 75% of visits were conducted via telemedicine. Reasons for failure to complete TCM are shown in Table 1. Regarding payment, of the successfully completed encounters, only six claims were denied by insurance payors and the remaining 94% (n=87) were reimbursed at a rate in keeping with other charges within our practice.
Conclusion(s):
Management of the critical time of transition from hospital to home is an essential function of Complex Care Programs. TCM CPT codes can be leveraged to ensure the financial viability of this time intensive process; telemedicine is a viable platform for these visits. Future studies will look at the effectiveness of our TCM program in preventing readmissions and in family self-efficacy and satisfaction.