Neonatal Quality Improvement
Neonatal Quality Improvement 6
 photo")
Leah F. Halpenny, MB BCh BAO, MSc (she/her/hers)
Fellow
BC Women's Hospital
Vancouver, British Columbia, Canada
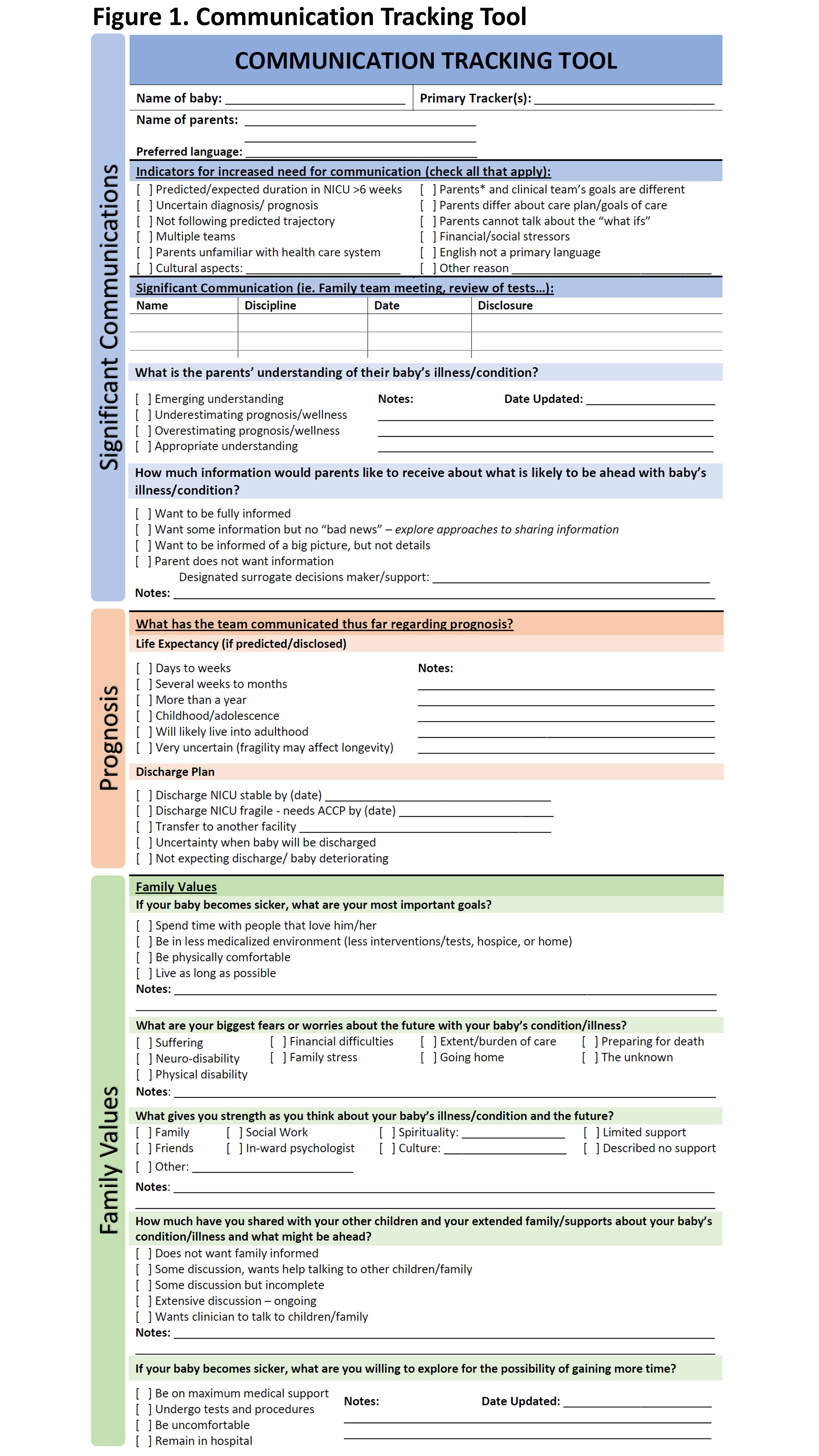
Communication in the Neonatal Intensive Care Unit can impact parental experience and outcomes, promote relationship building and information exchange, facilitate shared decision making, and empower families to advocate for their child’s care. As preterm babies are likely to remain in hospital for a prolonged duration, and may have an uncertain prognosis, integrating high-quality communication for these families can impact their overall experience. The Communication Tracking Tool (CTT) was previously developed to support communication in NICU (Fig 1). However, it had not been introduced to the preterm population of families.
The aim was to increase the occurrence of documented early communication episodes (≤ 96 hours) with families of premature infants to 80%. Our goal was that with earlier initiation and planning of values-based, family-centred communication, consistent high-quality communication would be established and maintained.
Quality improvement (QI) methodology was used to conduct this study. Cause and effect analysis determined contributing factors to current practice, and a driver diagram identified potential change ideas. Baseline data collection included family and staff surveys and chart review. Survey responses were compared to chart review data.
Following QI methods, Plan-Do-Study-Act (PDSA) cycles were conducted. A core intervention was the introduction of the CTT. Run charts were used to track use of the CTT and documented communication practice.
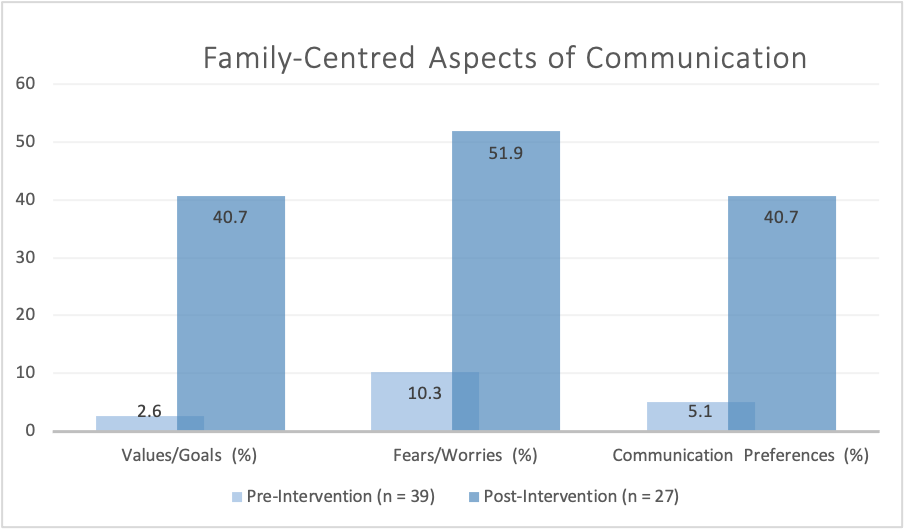
A key survey finding was a lack of consistency in communication. Additionally, while family and staff survey results suggested that some family-centred communication was taking place, chart review data revealed documentation did not reflect this (Fig 2).
Three PDSA cycles were completed. Interventions included introduction of the CTT, measures to promote its use, and education and knowledge translation sessions regarding family-centred communication and the CTT. To date, by using the CTT during early communication with families, documentation of topics such as communication preferences, values and fears, and sources of strength has improved, however practice remains varied.
We identified a need for increased family-integrated communication with families of preterm infants. A need for improved documentation regarding communication was also evident. Although we have not yet reached the targeted >80%, following three PDSA cycles there was an increase in documented family-centred communication (Fig 3). Ongoing work includes developing practical education sessions in use of the CTT.
.png)